AI in preventive medicine: What s already happening in (South) Africa

When I graduated from medical school 20 years ago, prevention was mentioned but never really taught. We were trained to find problems and fix them. Everything that qualified as true prevention, including guidance on diet, sleep, physical activity and stress, was left to dietitians, personal trainers, coaches and psychologists. The doctor’s domain was clear: does the patient have a disease or a disorder? And if so, how should it be treated?
That model has not fundamentally changed, but the world around it has.
Two trends over the past two decades
First, there was the app revolution. There’s now an app for everything, and apps have brought preventive health tools directly into people’s hands, no prescription required. Because these tools are classified as lifestyle rather than medical interventions, they sit largely outside regulatory oversight. The result is thousands of apps and AI-powered tools with wildly variable quality and very little guidance to help consumers distinguish what works from what does not.
The second trend is that people still regard their doctor as the Supreme Leader of Health. Many never reach a trained professional because the barrier is too high in terms of cost or effort. But for those who do, the consultation is a powerful moment. Doctors owe it to their patients to stay abreast of which consumer-grade tools have credible evidence behind them, and to be able to say: here is what has been tested, and here is what you can reasonably expect from it.
What is actually being deployed right now
Rather than speculating about what AI might one day do, I think it is more useful to look at what is already happening. Here are six examples I find genuinely instructive.
- AI chatbots for targeted patient populations
The first example comes from Audere, a non-profit company that has developed a suite of WhatsApp-based AI health companions, each operating within a tightly defined clinical domain. Coach Mpilo focuses specifically on HIV and TB, and is particularly valuable for people living with HIV who have interrupted their treatment and need consistent coaching to re-engage with care and maintain treatment adherence. VimbAI, deployed in Zimbabwe in partnership with CeSHHAR, supports users around HIV prevention and self-testing. Self-Cav, aimed at young South Africans, provides confidential guidance on sexual health, HIV, and mental wellbeing. Active research is underway to measure whether these tools improve linkage to care and viral suppression.
- Computer vision and audio signal processing for tuberculosis (TB) screening
Algorithms trained on digital X-rays can screen for TB with reasonable accuracy. The digital stethoscope from AI Diagnostics can do the same thing at roughly 1% of the cost of an X-ray machine, with comparable performance. In resource-constrained settings, which is most of the world, that cost difference matters enormously. Crucially, both technologies appear capable of detecting asymptomatic TB, which has significant implications for prevention of disease progression and onward transmission.
- Meal scanning and biometric monitoring
A South African company called Strove has built a corporate wellness platform, now also adopted by medical schemes, that allows users to photograph their meals for nutritional analysis. The friction of manually logging food, which most people abandon quickly, is largely removed. The same app includes a face scanning feature that infers heart rate and, to a lesser extent, blood pressure, using the same photoplethysmography principle as a smartwatch but at greater distance. Claims that it can accurately measure glucose and cholesterol levels are not yet sufficiently robust for clinical use. It is promising but still maturing.
- Predictive algorithms to prevent loss to follow-up
AMPATH, an academic consortium managing care for around 200,000 HIV-positive patients in Kenya, has built a super learner algorithm combining decision trees, neural networks and logistic regression to identify patients most likely to miss their next clinic visit. Support staff can then proactively reach out before the appointment is missed, keeping patients engaged and virally suppressed.
- AI-enabled diagnostic support for nurses
CareMate is a South African tool trained on the standard treatment guidelines for primary care, not through large language model techniques, but through a precise, rule-based approach. The innovation is in the translation layer: clinical questions are presented to patients in accessible, plain language, their responses are mapped back to clinical criteria, and the algorithm generates a differential diagnosis and recommendation. It also translates the output back into language the patient can understand. This is a thoughtful application of AI to extend the capacity of nurse practitioners.
- Ambient AI scribing
Akili AI is a MedTech platform that supports and augments the communication between healthcare professionals and patients. The platform records consultations, generates verbatim transcripts, and captures the underlying detail in a structured, retrievable manner, rather than locked inside a narrative. This makes it possible to automate the derivation of clinical notes and referral letters that integrate directly into electronic health records. As large language models improve, so will tools like this.
The prerequisite that is often overlooked
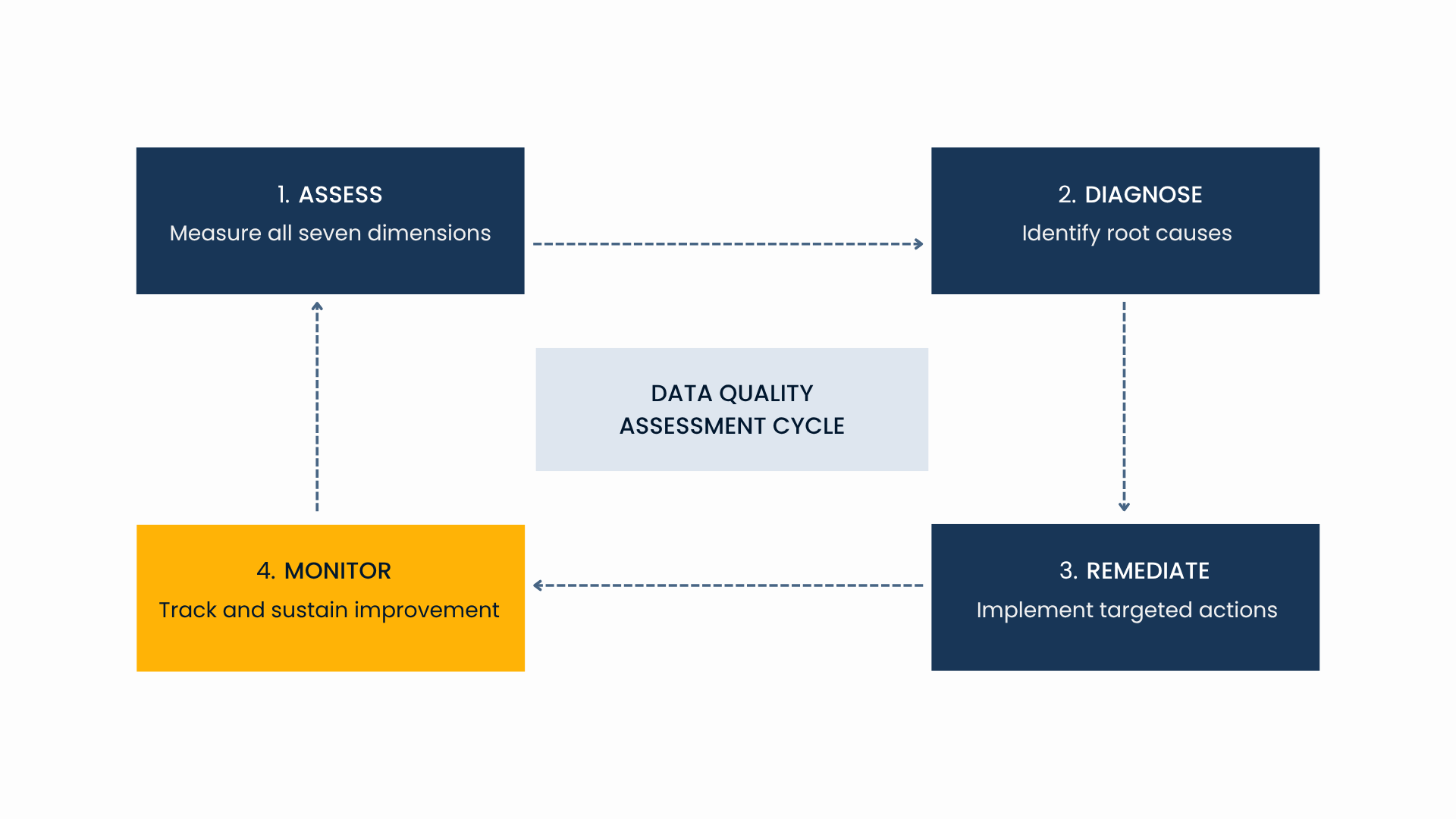
All of these applications depend on three things being in place: mature data infrastructure, strong data governance and high data quality. Without the first, development is slow, expensive and not scalable. Without the second, patient privacy is at risk and regulatory compliance cannot be guaranteed. Without the third, no inference drawn from the data is reliable. These are not optional conditions. They are the foundation on which any meaningful AI integration in healthcare is built.
The gap between what is technically possible and what is operationally real in healthcare is, more often than not, a data science challenge. Closing that gap requires people who understand both the clinical context as well as the interrelated domains of data infrastructure, governance, analytics and data quality. That is precisely the work we do at Wimmy, at the intersection of medicine and data science. If you are working on any of these challenges and would like to compare notes, I would be glad to hear from you.